Número: 9.9 - 7 Artigo(s)
- Imprimir
- Indicar
- Estatísticas
- (0) Comentários
- Como Citar
- Download Citação
- Artigos Relacionados
-
Outros dos Autores
- Diogo Machado de Oliveira
- Pedro Luiz Rodrigues Guedes
- Isabel Vieira De Assis Lima
- Laila Fieto Ribeiro
- Leonardo Figueiredo Vilela
- Luiz Alberto Barbosa
- Márcia Emília Moreira De Luca
- Beatriz Santos
- Ricardo Pessoa Martello Souza
- Tatiana Oliveira Fulco
- Valéria Salazar
- Sônia Cristina Leal Leidersnaide
- Plínio dos Santos Ramos
Artigos Originais
Aprendizagem baseada em problemas on-line como estratégia de ensino remoto emergencial no curso de Medicina durante a pandemia de COVID-19: Percepção e satisfação de aprendizagem
Online problem-based learning as an emergency remote teaching strategy in the medical course during the COVID-19 pandemic: Perception and learning satisfaction
Diogo Machado de Oliveira; Pedro Luiz Rodrigues Guedes; Isabel Vieira De Assis Lima; Laila Fieto Ribeiro; Leonardo Figueiredo Vilela; Luiz Alberto Barbosa; Márcia Emília Moreira De Luca; Beatriz Santos; Ricardo Pessoa Martello Souza; Tatiana Oliveira Fulco; Valéria Salazar; Sônia Cristina Leal Leidersnaide; Plínio dos Santos Ramos
1. MSc, Professor Adjunto da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
2. PhD, Professor Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
3. PhD, Professora Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
4. PhD, Professora Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
5. PhD, Professor Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
6. PhD, Professor Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
7. PhD, Professora Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
8. PhD, Professora Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
9. PhD, Professor Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
10. PhD, Professora Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
11. PhD, Professora Assistente, da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
12. PhD, Professora Assistente da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil
13. PhD, Diretor de Ensino, Pesquisa e Extensão da Faculdade de Ciências Médicas de Três Rios, FCM/TR, Brasil. E-mail: pliniosramos@gmail.com
Recebido em 09/02/2021
Aceito em 30/05/2021
Resumo
INTRODUÇÃO: O mundo foi brutalmente impactado por uma pandemia desencadeada pelo COVID-19. Como consequência, todo o planejamento pedagógico foi completamente desfeito.
OBJETIVO: O presente estudo teve como objetivo verificar a percepção de satisfação e aprendizagem dos alunos de graduação em medicina que foram expostos à implementação do Ensino Remoto Emergencial (TRE) com Aprendizagem Baseada em Problemas Online (O-PBL).
MÉTODOS: Cento e vinte e seis estudantes participaram do estudo. A implementação do TRE com O-PBL teve como objetivo trabalhar exclusivamente conteúdos teóricos cognitivos e correspondeu a um período total de 8 semanas. Foram feitas perguntas específicas para quantificar a percepção de satisfação e aprendizado por meio de uma pontuação de 0 a 10 em cinco momentos de todo o processo. Foi realizada análise estatística e obtidas as médias dos escores globais, bem como os respectivos intervalos de confiança de 95%.
RESULTADOS: As avaliações perceptivas gerais mostraram um alto nível de satisfação e aprendizado em todos os momentos. Todos os grupos relataram escores semelhantes de percepção de satisfação para o conjunto de atividades relacionadas ao processo (1º período 8,8 ± 0,23 escore; 3º período, 8,8 ± 0,35 escore; 4º período, 8,71 ± 0,12 escore, P > 0,05). Para o conjunto de atividades relacionadas ao aprendizado, o 1º período apresentou nota inferior, 7,78 ± 0,31 em relação ao 3º período, 8,37 ± 0,19 escore, P < 0,05, e para o 4º período, 8,44 ± 0,24 escore, P < 0,01.
CONCLUSÃO: A implementação simultânea do TRE com O-PBL possibilitou a continuidade e manutenção do processo ensino-aprendizagem com alta percepção de satisfação e aprendizagem dos alunos.
Palavras-chave: Educação Médica; Aprendizagem Baseada em Problemas; Ciências da Saúde
INTRODUCTION
In March 2020, the world was brutally impacted by a pandemic unleashed by COVID-19 [1]. The widely used strategy to contain the spread of contamination was to adopt social isolation, aiming to have minimal contact between human beings [2]. From that moment on, human relations and activities were drastically altered [2]. In this context, the face-to-face contact between teachers and students, which is extremely important for the quality of teaching in medical education, was, at first, severely hampered by social distance, and consequently, all pedagogical planning had been completely undone [3,4].
Implementation of an emergency teaching method was necessary. Universities and colleges have adopted Emergency Remote Teaching (ERT) as a method that is characterized by remote teaching solutions for instruction or education that would be delivered in person [5]. The main difference between ERT and Online Learning is that the aim of ERT is not to re-create a robust educational ecosystem, but rather to provide temporary access to instruction in a manner that is quick to set up and is reliably available during an emergency or crisis[6]. Although ERT is based on offering remote facilities, its implementation and accession within an educational system can be considered a complex task due to some factors. First, the time for training and adaptation is extremely short; second, it requires a very high level of organization and integration between directors, teachers, employees, especially the information technology department, and students about the measures adopted by the institutions; third, convincing the students to trust in the new teaching-learning process is essential [7].
Another challenging factor faced by educational institutions is associating the implementation of ERT with the previously established learning method. A strategy created in 1980, called Problem Based Learning (PBL), revolutionized medical education and nowadays it is used in several health courses [8,9]. The method philosophy consists of the education general strategy focused on self-directed learning, small group discussion with facilitators, and working through problems to acquire knowledge. PBL is a strategy pedagogical student-centered that aims to integrate the knowledge of the basic sciences to the medical clinic, where is necessary for all participants, tutors, and students, to follow precise stages for the method to be effective. However, the implementation of ERT with PBL is a complex task because it involves multiple factors and requires a high interaction between all members.
Thus, this study aimed to investigate the satisfaction perception and learning of the undergraduate medical students that were involved in the ERT implementation and integration with O-PBL during the period of social isolation due to the COVID-19 pandemic. The hypothesis is that the ERT associated with Online PBL (O-PBL) could be an effective emergency strategy in the manutention of quality in the teaching-learning of the undergraduate medical students.
AIM
The present study aimed to Investigate the satisfaction perception and learning of the that were involved in the ERT implementation with O-PBL during the period of the COVID-19 pandemic.
METHODS
Subjects
The educational intervention study was conducted at the Faculty of Medical Sciences of Três Rios (SUPREMA), Três Rios, Rio de Janeiro, Brazil. This new faculty started its academic activities in August 2018. In this sense, the study comprised an evaluation of all regularly enrolled students, containing a total of one hundred and twenty-six students bachelor of medicine, subdivided to the 1st period (53 students); 3rd period (48 students); and 4th period (25 students). Eligibility criteria were as follows: the students needed to have participated in the entire O-PBL process. The consent verbal was obtained from all participants and the study was conducted in accordance with the Declaration of Helsinki [10,11].
ERT implementation with O-PBL
ERT implementation and integration with O-PBL aiming to work exclusively on cognitive theoretical content started on May 4th, 2020. Students were separated into small groups, containing a maximum of twelve students per group [12]. The week of activities was programmed as follows: Week one: on Monday morning the students received the “case problem” at 7:00 am and it was opened at 09:00 am, by the respectively responsible tutor; on Tuesday, Wednesday and Thursday the students participated in supports stations with teachers. These stations were carried out asynchronously and synchronously, with a maximum duration of forty minutes and twenty students per support station [13]; on Friday morning, the students sent individual manuscript copies by email with the researched sources of their studies for each of the learning issues raised at the “opening of the case”. The deadline for submitting responses was until 9:00 am, and at 9:01 am the tutor responsible for each group of students started the “closing of the case”, ending it at noon. Week two: students received study guides with theoretical contents and learning objectives about each of the subjects of their course period. Also, students received a timetable to schedule a conference with teachers to clarify doubts. This two-week cycle was repeated four times, totaling 8 weeks. ZOOM platform was used to deliver all educational sessions. Table 1 shows the ERT implementation stages with O-PBL.

Assessment of satisfaction perception and learning
At the end of each week of application of the O-PBL, the perception of satisfaction and learning was assessed through an anonymous questionnaire completed on the Google Forms platform. Specific questions were asked to quantify through a score of 0 - 10 five moments of the entire process: First meeting; Supports stations; Last meeting; and Set of activities (process and learning). Table 2 shows the description of the questions with their respective answer options included in the evaluation questionnaire.

Assessment of ERT implementation with O-PBL
The ERT evaluation with O-PBL occurred through specific questions that intended to assess the ease of connection, quality, and suitability of the platform and aspects such as transmission quality (sound and image). Also, a question was asked to assess whether tutors performed all the steps that consist of the O-PBL method. Assessment ERT with O-PBL aimed to evaluate only the moments: First meeting; Support stations and Last meeting. Table 2 shows the description of the questions with their respective answer options included in the evaluation questionnaire.
Statistical analysis
The data referring to scores of first meeting; support stations; last meeting; and set of activities (process and learning) were grouped on average at the end of two, four, six, and eight weeks. Data distribution was tested by Shapiro-Wilk’s test. The data were analyzed by two-way repeated-measures ANOVA. The Bonferroni Posttests was used after ANOVA if needed. All analyses were done using the software GraphPad Prism (version 5.00). Results are reported as the mean and standard error of the mean and the differences between scores were considered statistically significant if the probability of differences occurring by chance alone was less than 0.05.
RESULTS
Satisfaction perception and learning
Overall perceptual assessments showed a high level of satisfaction and learning at all moments during the ERT implementation with O-PBL. All periods reported similar scores of satisfaction perception for the set of activities related to the process (1st period, 8.8 ± 0.23 score; 3rd period, 8.8 ± 0.35 score; 4th period, 8.71 ± 0.12 score, P > 0.05). For the learning perception for the set of activities related to the process, the 1st period presented a lower score, 7.78 ± 0.31, compared to the 3rd period, 8.37 ± 0.19 score, P < 0.05, and to the 4th period, 8.44 ± 0.24 score, P < 0.01.
The assessment regarding the first meeting showed a high score of all periods, where the 1st period (9.43 ± 0.11 score) reported the highest score compared to the 3rd period (8.88 ± 0.07 score, P < 0.05) and similar score compared to the 4th period (9.24 ± 0.10 score, P > 0.05). The assessment support stations and the last meeting showed a similar and high satisfactory score in all periods. Figure 1 shows the results of satisfaction perception and learning score of all periods at different stages of implementing ERT with O-BPL.
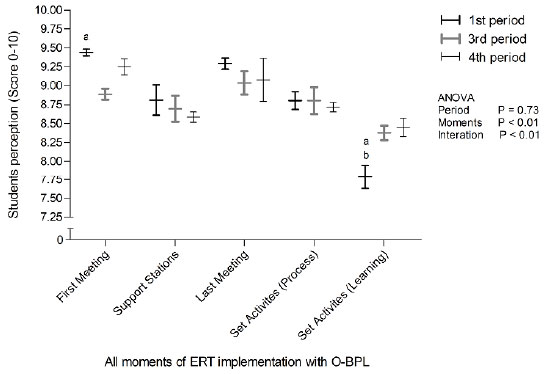
Figure 1. Satisfaction perception and learning score of 1st period (thick black line), 3rd period (thick gray line), 4th period (thin black line), at different stages of implementing ERT with O-BPL. Data analyzed by two-way ANOVA, followed by the Bonferroni post hoc, if needed. aP < 0.05 1st period versus 3rd period within moment; bP < 0.01 1st period versus 4th period within moment.
ERT Implementation with O-PBL
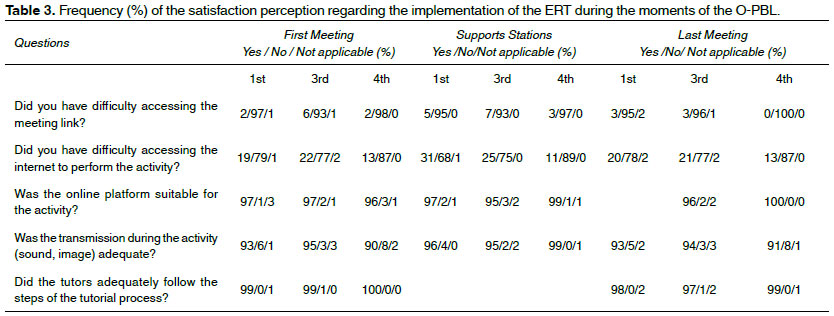
The first observed factor was a very low percentage of students with difficulty in accessing the meeting link, the highest percentage being only 7% reported up to the 3rd period in the support stations. The greatest difficulty faced by students was related to access to the internet to carry out the proposed activities, where the highest percentage was 31% reported by the 1st period at the support stations (Table 3). All periods reported that online platforms suitable for activity (1st period: 97%, 3rd period: 96%, 4th period: 98%) and quality of transmission (above 90% in all periods) were adequate during the activities at all moments of the process. Moreover, the 1st and 4th periods were unanimous in a report that tutors adequately follow the steps of the tutorial process. Table 3 shows the frequency (%) of the satisfaction perception regarding the implementation of the ERT during the moments of the O-PBL.
Discussion
Until the moment, we know that any ERT strategy will not replace the effectiveness of presential teaching. However, looking for alternatives that are similar to the methods already experienced by students when we are in an atypical moment seems to be the most effective way to try to offer quality teaching. The option to work with active methods and in small groups is in line with the national curriculum guidelines for teaching medicine in Brazil and allowed us to get closer to the activities carried out at our institution [14]. In this sense, was appropriated to verify the students perception regarding the use of ERT with O-PBL for the cognitive theoretical contents.
As a main result, we evidence that overall perceptual assessments showed a high level of satisfaction and learning at all moments during the implementation of ERT with O-PBL. In the same sense, Shim et al. (2020)[15] demonstrated that ERT is an improved system maintaining academic achievement similar to the traditional classroom when applied correctly and guaranteeing some fundamental aspects for its implementation. These consist basically of three aspects: 1) technology and infrastructure, 2) the facilitator; including quality of facilitation and facilitator expertise, and 3) group dynamics; including ground rules, roles, responsibilities, and learning style[16].
The technology aspect was contemplated since a very high percentage of all periods reported that the online platform suitable for the activity and the quality of the transmission (sound and image) was adequate during the activities in all moments of the process. The second aspect attended was the quality of the facilitator, evidenced by the unanimous report of 1st and 4th period that tutors adequately follow the steps of the tutorial process (Table 3). We emphasize that all tutors received training and instructions before starting to apply the PBL method. The third aspect is directly related to aspects that characterize the PBL method and its ability to be adapted to preserve its benefits from an active learning methodology [17,18].
The 1st period reported a lower score of perceptions of learning when compared to other periods, which could be explained by the lack of experience and familiarity with the method since the 1st period had only one week of adaptation with O-PBL in person. We emphasize that the differences found in evaluations by course periods did not surprise us, since those were students who had just entered medical school and were not yet familiar with the method.
One aspect not available in this study, but observed by the teachers and reported by the students, was the great fatigue related to the process at the end of 8 weeks. The exacerbated increase in fatigue at the end of the process may have a direct correlation across all interactions depending only on virtual contact and consequently accumulated hours in front of the computer [19,20]. According to Bao (2020) [21], adjusting the pace of online classes can reduce concentration issues along with being able to deliver class content more effectively. Even with the perception of tutors and preceptors that students were reporting more tired to carry out proposed activities, nevertheless, the fact did not reflect on the perception of students about satisfaction and learning with the method adopted.
ERT implementation with O-PBL included only theoretical cognitive content, once all practical content will be restored when the safety conditions of teachers and students are reestablished. However, some processes offer students the opportunity to practice obtaining a patient history, differential diagnosis, clinical reasoning, and patient management skills from a remote environment [22].
A possible limitation of this study could be attributed to the pre-established responses present in the questionnaire, which could induce and limit the students perception of the process. It is necessary to conduct studies that quantify learning robustly and directly through the ERT implementation with O-PBL.
CONCLUSION
The simultaneous ERT implementation with O-PBL enabled the continuation and maintenance of the teaching-learning process with a high perception of student satisfaction and learning during the COVID-19 pandemic.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study did not require formal approval from the ethics committee local (Faculty of Health and Medical Sciences - SUPREMA), but strictly followed the standards of ethical principles of medical research included in the Declaration of Helsinki. The researchers signed a term of commitment to use the data, to safeguard all the individuals evaluated and their personal information in the face of any means of communication. Limiting still to use only the data necessary only for the development of this manuscript, this being a responsibility assumed by the responsible researcher.
ACKNOWLEDGMENT
The authors are grateful to the students who trusted all the decisions adopted by the coordination of the faculty and in special the secretary of coordination Rafaela Ribeiro Soares and the information technology technician Pedro Henrique Victor Teixeira who were essential to logistical support during the ERT implementation with O-PBL.
REFERENCES
1. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. Journal of autoimmunity. 2020;1024-33
2. Smith BJ, Lim MH. How the COVID-19 pandemic is focusing attention on loneliness and social isolation. Public health research & practice. 2020;1-4
3. Ahmed H, Allaf M, Elghazaly H. COVID-19 and medical education. The Lancet Infectious diseases. 2020;777-8
4. Sandhu P, de Wolf M. The impact of COVID-19 on the undergraduate medical curriculum. Medical education online. 2020;1764740
5. Kaiper-Marquez A, Wolfe E, Clymer C, Lee J, McLean EG, Prins E, et al. On the fly: Adapting quickly to emergency remote instruction in a family literacy programme. International review of education Internationale Zeitschrift fur Erziehungswissenschaft Revue internationale de pedagogie. 2020;1-23
6. Connolly C, Hall T. Designing for emergency remote blended and online education: a response to Bennett et al. (2017). Educational technology research and development : ETR & D. 2020;1-4
7. Gaur U, Majumder MAA, Sa B, Sarkar S, Williams A, Singh K. Challenges and Opportunities of Preclinical Medical Education: COVID-19 Crisis and Beyond. SN comprehensive clinical medicine. 2020;1-6
8. Tudor Car L, Kyaw BM, Dunleavy G, Smart NA, Semwal M, Rotgans JI, et al. Digital Problem-Based Learning in Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. Journal of medical Internet research. 2019;129-45
9. Bassir SH, Sadr-Eshkevari P, Amirikhorheh S, Karimbux NY. Problem-based learning in dental education: a systematic review of the literature. Journal of dental education. 2014;98-109
10. Hurst SA. Declaration of Helsinki and protection for vulnerable research participants. Jama. 2014;1252
11. Hellmann F, Verdi M, Schlemper BR, Jr., Caponi S. 50th anniversary of the Declaration of Helsinki: the double standard was introduced. Archives of medical research. 2014;600-1
12. Pichon-Riviere E. Family groups: An operative approach [Grupos familiars: Un enfoque operativo]. Del Psicoanalisis a la Psicologia Social. 1971;202-13
13. Robert M. Bernard PCA, Eugene Borokhovski, C. Anne Wade, Rana M. Tamim, Michael A. Surkes, and Edward Clement Bethel. A Meta-Analysis of Three Types of Interaction Treatments in Distance Education. Review of Educational Research. 2009;1243-89
14. Meireles MAdC, Fernandes CdCP, Silva LSe. Novas Diretrizes Curriculares Nacionais e a Formação Médica: Expectativas dos Discentes do Primeiro Ano do Curso de Medicina de uma Instituição de Ensino Superior. Revista Brasileira de Educação Médica. 2019;67-78
15. Shim TE, Lee SY. College students experience of emergency remote teaching due to COVID-19. Children and youth services review. 2020;105578
16. Davies R, Yeung E, Mori B, Nixon SA. Virtually present: the perceived impact of remote facilitation on small group learning. Medical teacher. 2012;676-83
17. Yan Q, Ma L, Zhu L, Zhang W. Learning effectiveness and satisfaction of international medical students: Introducing a Hybrid-PBL curriculum in biochemistry. Biochemistry and molecular biology education : a bimonthly publication of the International Union of Biochemistry and Molecular Biology. 2017;336-42
18. Hung W, Dolmans D, van Merriënboer JJG. A review to identify key perspectives in PBL meta-analyses and reviews: trends, gaps and future research directions. Advances in health sciences education : theory and practice. 2019;943-57
19. Ranasinghe P, Wathurapatha WS, Perera YS, Lamabadusuriya DA, Kulatunga S, Jayawardana N, et al. Computer vision syndrome among computer office workers in a developing country: an evaluation of prevalence and risk factors. BMC research notes. 2016;150
20. Rosenfield M. Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2011;502-15
21. Bao W. COVID-19 and online teaching in higher education: A case study of Peking University. Human behavior and emerging technologies. 2020;113-5
22. North R, Vitto C, Hickam G, Santen SA. Remote Learning in the Time of COVID-19. AEM education and training. 2020;280-3

